
Providers close care gaps year-round with the right data
Accelerate your HEDIS gap closure rates by enabling provider groups with predictive analytics and real-time member insights.





Provider groups are the execution layer for care gap closure, but they routinely operate without the member-level attribution and gap visibility required to take action at the point of care.
Missed care gaps impact quality performance and financial performance by lowering HEDIS® scores and Star Ratings. For most health plans, the barrier to closing care gaps and improving quality performance is workflow design. Providers receive aggregate reports when they need patient-level lists, plan-level summaries when they need practice-specific rosters, and generic outreach when they need targeted, measure-specific guidance tied to incentive opportunities.
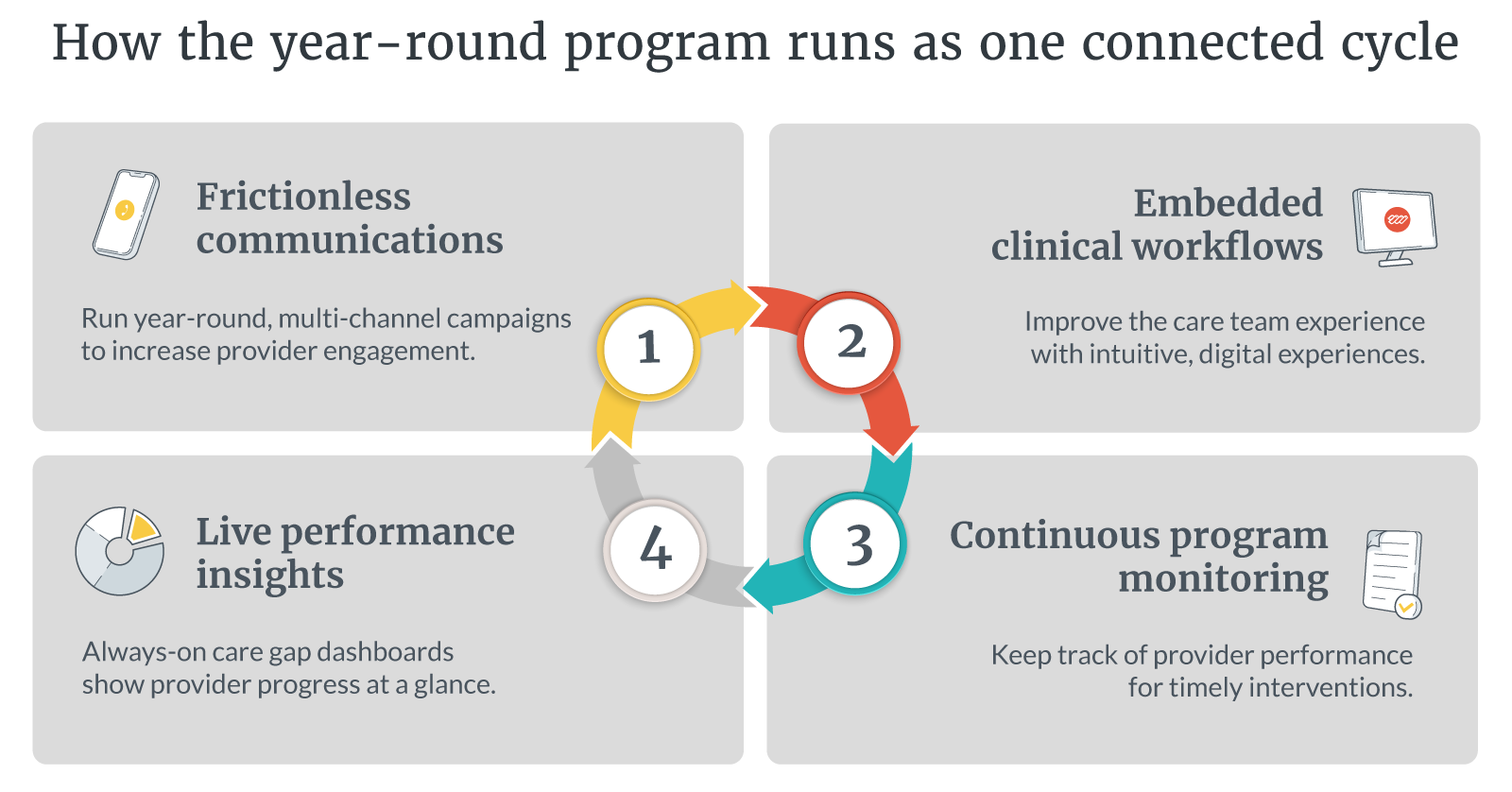
Care gap management software can address the coordination failure directly. It gives provider groups attributed member views, gap-level detail, and the timeline context that makes prioritization possible. This, combined with visible incentive tracking and omnichannel engagement, give providers the context to act during a patient encounter, well in advance of quality deadlines. Care gap management becomes a year-round program that health plans can administer continuously without introducing friction to existing workflows.
The reasons care gaps go unclosed year after year
Care gaps go unclosed when providers receive aggregate quality reports rather than patient-level lists. Without attributed member views, a colorectal cancer screening rate cannot be converted into a prioritized list of specific patients who need action before the measure window closes.
Fragmented data compounds the problem. Health plans running quality programs across disconnected systems produce care gap lists that providers may find inconsistent with their own EHR records, eroding trust over time. Health plans then default to a concentrated year-end push that consistently produces subpar results.
Physicians and their staff spend an average of fifteen hours per week on care gap closure and quality measure activities, yet plans that rely on seasonal campaigns absorb that effort in the least productive period of the quality calendar. When plans deliver providers highly accurate data, in real time, and connected to the workflow providers already use, they can improve provider engagement and increase care gap closure rates.
Give providers the patient panel behind the percentage
Providers need to be able to log into a single, EHR-connected portal to see their individual patient panel, the specific open quality and risk gaps for each member, the measures at stake, and the evidence submission workflow. The plan configures the program; the portal keeps the provider view current as gaps close and new members are attributed, without requiring the plan to prepare or distribute roster files manually.
The difference between an aggregate measure report and an attributed member list is the difference between knowing that colorectal cancer screening performance is at sixty-two percent and knowing which forty-seven patients in a specific practice are overdue for that screening. Providers need patient-level precision in order to act on care gaps year-round.
AI care gap identification surfaces predictive HEDIS quality gaps
AI-enabled care gap identification surfaces predictive HEDIS quality gaps by analyzing member data to flag patients likely to end the measurement year with open gaps. It gives providers the data they need to act well in advance of reporting deadlines, surfacing insights based on patients’ care trajectory, chronic condition profile, and utilization patterns. Provider groups receive these predictive signals alongside confirmed gaps, giving them a prioritized work list that reflects both where performance has already slipped and where intervention can still prevent it from doing so.
Plans that work predictive gaps in Q1 and Q2 distribute closure activity across the year, improve provider response rates, and carry less Star Ratings risk as measure windows approach. Plans that work only confirmed gaps in Q4 face the shortest timelines and the least flexibility to course-correct before submission.

Making incentive dollars visible at the point of action
Health plans running incentive programs through spreadsheets or opaque post-period true-ups are missing an opportunity to earn provider trust through incentive visibility. Integrating incentive data directly into the provider workflow gives provider groups visibility into year-to-date earnings, remaining incentive opportunity, and performance against contract targets in the same portal where they review attributed members and submit gap closure evidence. The financial context sits adjacent to the clinical list, connecting the action to the compensation it generates without requiring the provider to navigate to a separate system or wait for a quarterly report.
When the dollars are visible at the point of action, practice administration may allocate more consistent attention to gap closure, and providers can see how their actions directly generate resources for their practice.
Year-round provider engagement without abrasion
The frequent cause of failure in provider quality programs is abrasion: too many portals, too many conflicting gap lists, and too much generic outreach. Health plans managing quality through disconnected systems accumulate provider fatigue over time, reducing response rates and portal adoption until the program depends entirely on a narrow set of already-engaged practices.
Coordinating payer-to-provider quality communication via weekly summary emails, in-app notifications, and measure-specific campaign messages supports a year-round approach to care gap closure. Communication routes through one system tied to the same gap lists and incentive data providers see in the portal. Outreach targets open gaps and non-responders rather than the full network, reducing noise for engaged practices and applying structured follow-up where response rates are low. Provider groups that receive consistent, relevant communications sustain engagement across the full measurement year rather than responding only when year-end pressure accumulates.
Preparing for HEDIS 2027 measure changes with a year-round program
Each HEDIS measurement year brings new measure specifications, updated denominator criteria, and retired measures, and the HEDIS 2027 updates expected later in 2026 will require health plans to adapt their gap closure workflows again. Plans operating year-round workflows can absorb those changes without rebuilding provider engagement from scratch. The infrastructure, including the provider relationships, portal adoption, and communication cadence, already exists and runs continuously.
Each year of continuous operation improves the program: practices become more familiar with the workflow, trust the gap data more consistently, and require less outreach to generate the same closure activity. Plans that invest in a year-round program in 2026 enter the 2027 measure cycle with a provider engagement model already calibrated to absorb change, rather than one built from reactive outreach during HEDIS season.
Closing care gaps starts with giving providers what they need
Care gap closure is a coordination problem as much as a clinical one. Provider groups that have attributed member views, predictive HEDIS quality gap signals, visible incentive tracking, and coordinated communications from payers can act continuously and consistently across the measurement year.
Reveleer Care Gap Manager connects payers and provider groups around a shared, real-time view of attributed members, open quality and risk gaps, and the evidence workflows required to close them. Health plans using Care Gap Manager benefit from:
- Attributed member views at the practice level, giving provider groups the patient-specific gap detail needed to act before measure windows close
- AI-driven predictive gap identification that surfaces members at risk of non-compliance earlier in the measurement year, when intervention is still clinically and operationally feasible
- Integrated incentive tracking that makes year-to-date earnings and remaining opportunity visible in the same portal where providers review gaps and submit evidence
- Omnichannel provider outreach coordinated across measures, lines of business, and contract types through a single system, reducing abrasion and improving response rates year-over-year
- Always-on dashboards that give health plan administrators real-time visibility into provider performance, gap closure progress, and program ROI
Reveleer customer data shows that plans using Care Gap Manager report up to 40% higher supplemental data submissions from provider groups and measurable improvements in HEDIS® measure performance and Star Ratings. To move from reactive quality management to a year-round quality program, connect with Reveleer to see how the Care Gap Manager can perform across your specific line of business and provider network.

Closing Care Gaps FAQ
What is a care gap?
A care gap is a missed or delayed clinical action that affects a patient's quality measure performance, such as a colorectal cancer screening or annual wellness visit not completed within the measurement year. Open care gaps lower HEDIS scores and Star Ratings, which is why health plans work to close them throughout the year rather than during a year-end push.
What is HEDIS®?
HEDIS (Healthcare Effectiveness Data and Information Set) is the quality measurement standard most health plans use to assess performance across clinical, patient experience, and utilization measures. HEDIS results feed Medicare Advantage Star Ratings, tying quality measure performance directly to plan revenue and member growth. HEDIS® is a registered trademark of the National Committee for Quality Assurance (NCQA).
What is the most effective strategy for HEDIS gap closure?
The most effective strategy transitions from retrospective data to real-time, shared data visibility between payers and provider groups, paired with automated incentive tracking.
How do you close care gaps without provider abrasion?
By using omnichannel provider outreach that coordinates all open measures and lines of business through a single, unified workflow portal.
About the Author

Related Resources

The ROI of AI-enabled prospective risk adjustment
Learn how AI-enabled prospective risk adjustment drives better clinical outcomes, reduces costs, and improves value-based care.

Ethical AI in value-based care: Balancing innovation with trust and transparency
Watch the session, ‘Ethical AI in Value-Based Care’, to learn about Reveleer’s AI trust and transparency.

Simplifying HEDIS®: How intelligent automation gives you more time
Learn how intelligent automation accelerates HEDIS reporting, improves efficiency, and enhances data accuracy for healthcare organizations.