
Provider abrasion starts with duplicate chart retrieval
How a centralized clinical data repository reduces provider abrasion by eliminating duplicate chart retrieval.




Health plans ask provider organizations for the same clinical documentation every day across risk adjustment, quality, audit, and care management programs. In many organizations, chart retrieval still moves through disconnected workflows with limited visibility into records already collected elsewhere in the enterprise.
Provider offices may receive repeated requests for the same charts from different teams within the same health plan, while payer staff spend additional time locating and reconciling documentation already gathered during earlier reviews. Repeated chart requests increase provider abrasion, raise retrieval costs, and slow RADV preparation, HEDIS abstraction, quality review, and care gap analysis across payer operations.
Why duplicate retrieval persists
Risk adjustment and quality teams often rely on the same clinical documentation, but many health plans still manage chart retrieval through separate vendors, storage systems, and departmental workflows. Risk adjustment programs retrieve charts to support coding accuracy, retrospective submissions, and RADV audits, while quality teams use clinical records for HEDIS abstraction, STAR measure review, and care gap closure initiatives. A chart retrieved for retrospective risk adjustment review may later be requested again for HEDIS abstraction or care gap review because the documentation remains tied to an earlier retrieval project or audit.
Most health plans still organize clinical documentation around projects and audits rather than maintaining a longitudinal member record. Once a retrieval effort closes, charts may remain archived inside departmental repositories or vendor systems that other teams cannot easily search or access. Teams initiating new retrieval efforts often have limited visibility into records already collected elsewhere in the organization.
The cost of fragmented chart retrieval
Duplicate retrieval increases operational cost across payer organizations. Health plans pay retrieval fees, vendor charges, and staff time for the same documentation multiple times across risk adjustment and quality programs because prior records often remain difficult to identify before new retrieval begins. Provider organizations also absorb additional administrative burden as repeated requests arrive from multiple teams within the same health plan.
Research published in the National Library of Medicine linked inaccessible prior records to duplicated tests and treatment delays that added an average of approximately $1,100 per patient to care costs. Similar inefficiencies appear inside payer operations when clinical documentation remains fragmented across retrieval systems, archived projects, and disconnected departmental workflows. Teams preparing for RADV response, HEDIS abstraction, quality review, or care gap closure initiatives often spend substantial time locating and reconciling records before clinical review can begin.
The differences between project-based chart management and centralized clinical record management extend across several operational areas:
Building a longitudinal clinical record
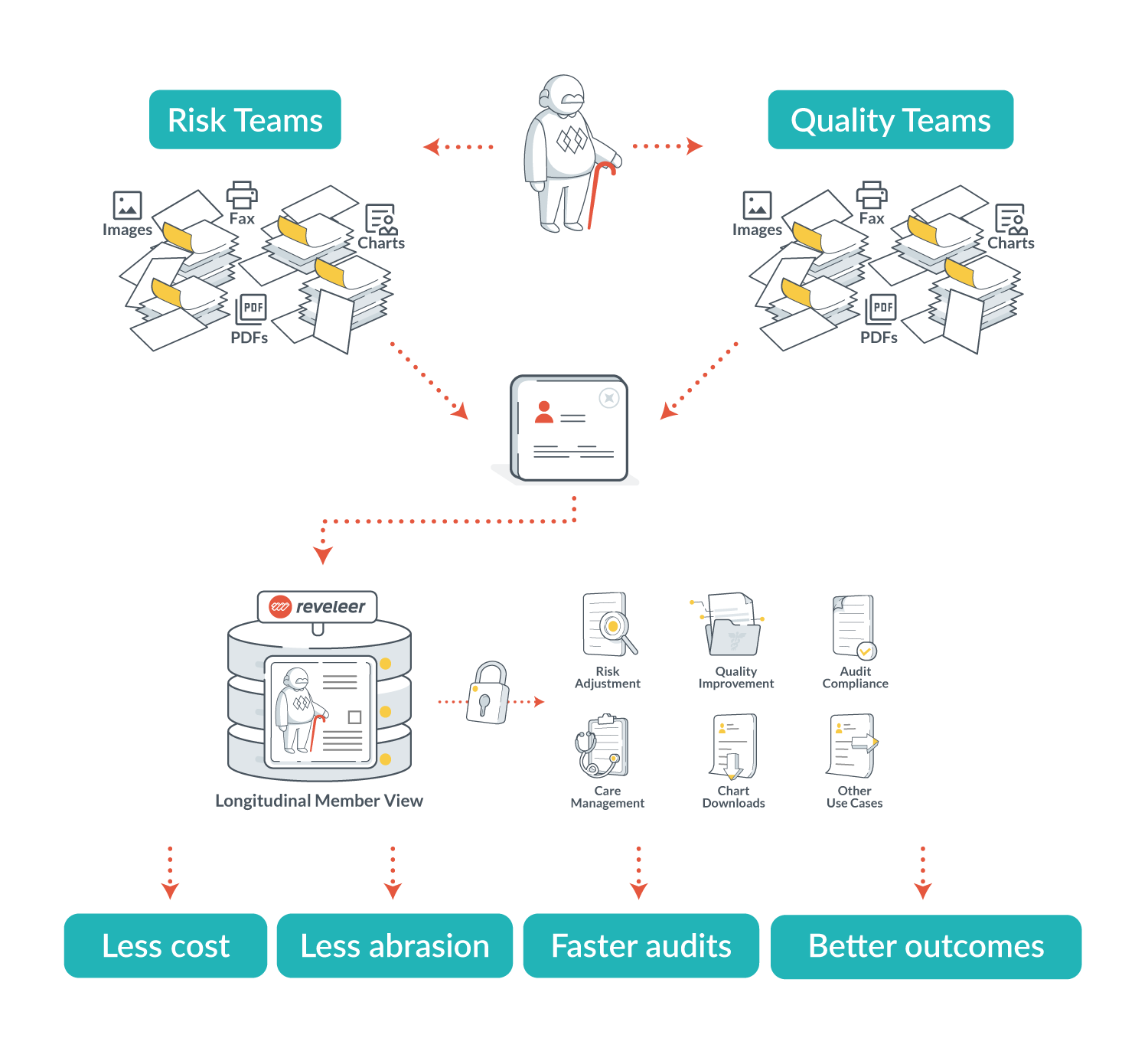
A centralized clinical data repository (CDR) stores charts at the member level independent of any single project, department, or vendor environment. Clinical documentation remains connected across payer workflows over time, allowing risk adjustment, quality, audit, and care management teams to reference the same longitudinal member record instead of rebuilding chart inventories for each initiative.
OCR and natural language processing (NLP) technologies extract metadata including member identifiers, provider information, dates of service, document types, and chart attributes. Standardized indexing allows teams to locate records across retrieval and audit workflows without manually searching archived projects, disconnected vendor systems, or departmental repositories.
Role-based permissions and audit trails allow organizations to manage access to clinical documentation while maintaining oversight across operational and compliance workflows. Teams can reference shared clinical evidence while maintaining appropriate controls around access and evidence management.
How centralized records change payer operations
Payer organizations can review existing documentation before launching new retrieval activity when clinical records are maintained through a centralized repository. Risk adjustment, quality, audit, and care management teams can work from the same longitudinal member record rather than maintaining separate chart inventories across departmental workflows.
Centralized record management reduces duplicate outreach to provider offices already managing large volumes of payer requests. Health plans also reduce retrieval expense and reconciliation work tied to redundant chart collection. Teams can reference the same longitudinal member record without rebuilding separate chart inventories across departmental workflows.
Reassessing fragmented payer workflows
Many health plans cannot quantify how often risk adjustment and quality teams retrieve the same documentation across separate workflows until retrieval activity is evaluated across both functions. Many payer organizations still organize clinical documentation around projects and departmental workflows instead of maintaining longitudinal member records.
As RADV scrutiny, retrieval volume, and cross-functional dependence on clinical evidence continue to increase, payer organizations may need to reevaluate how documentation moves across risk adjustment, quality, audit, and care management programs. Centralized clinical data repositories offer one approach to reducing provider abrasion while improving visibility into clinical records already on file across payer operations.
Health plans evaluating how clinical records move across risk adjustment, quality, and audit workflows can connect with Reveleer to assess the operational impact of fragmented chart retrieval and project-based storage models, or schedule a demo to explore a more scalable and reusable approach to clinical data management.

About the Author
Related Resources

Heading
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
Heading
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
Heading
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.